Perspectives on New
Information Technologies for VHA
Prepared for
Business
Veterans Health Administration
Department of Veterans Affairs
Tom Munnecke
Science Applications International Corporation
(858) 756 4218
Available at http://www.munnecke.com/papers/D21.doc
Table of
Contents
Comparison
of Hailstorm with original DHCP design concepts
Comments
on SOAP, XML, and DHCP Kernel Architectures
Industry
Controversy over HailStorm Architecture
Patient
Flow vs. Provider Flow
2. Health and the Network Effect
A
Spectrum of Health Activities
How
Cost/Benefit Analysis can Override Human Values
Limits
of Economic Analysis of Health Care
3. Complementary Currencies for Health
VHA
Health Bucks: A Scenario for a VA Complementary Currency
Appendix
A: Microsoft HailStorm Architecture
Appendix
B: VHA Voluntary Timekeeping Software
System
Appendix
C: A Peer to Peer Health Care System
Introduction
The pace of technical innovation in the information and technology industry over the past decades has been dramatic and accelerating. The typical automobile on the road has more computing power than the Apollo Lunar Landers. The initial PDP 11 computers used to support DHCP in 1983 used a “high speed” Unibus to connect the computer and its internal memory at a distance of a few inches. Today, patients can access the Internet via cable modems at a faster rate, from anywhere in the world.
Although it is impossible to predict exactly what will happen in the next 5-8 years, we can be sure that the growth in computing and communications capabilities will continue dramatically. These capabilities will not only make current information systems faster and less expensive, but they will also create fundamentally new ways of thinking about the way organizations use these technologies. The purpose of this paper is to describe some of these technologies and ways of viewing them through fresh perspectives.
The emergence of Amazon.com could not be understood from the perspective of bookstores in shopping malls, nor could Napster be understood from the perspective of the music industry. Similarly, the effects of new internet and communications technologies cannot be understood from the perspective of the current health care system. These changes may be not necessarily be “friendly” growth paths; they may require some major changes in standard patterns of thinking. Nevertheless, they are important to consider when dealing with technology innovation.
Some of these perspectives are:
- Intense Internet growth moves to the “edge” of the net, focusing on individuals rather than web servers. Peer to peer (P2P) architectures change the technical landscape, sometimes inverting the role of enterprises and individuals. (see Appendix C) Individuals become the center, surrounded by the enterprises which provide services to them. Section 1 describes Microsoft’s HailStorm technology is a leading candidate to play this role, which creates both opportunities and concerns for future VHA information architectures.
- The scale and interactivity of these technologies creates new opportunities to use them for VHA health activities. In order to do so, we need to look at health from a broader perspective, including preventative health as well as new forms of trust and community formation. Section 2 discusses health and the network effect.
- Complementary currencies – such as frequent flier mileage programs – are becoming easier to create with modern information technology. One way to build community and overcome accounting difficulties is to define a complementary currency for Veteran’s Health. A scenario for creating “VHA Health Bucks” as a complementary currency for health is discussed.
1. Inverting Perspective
The VHA Enterprise Architecture is, by definition, an enterprise-focused perspective of information technology within VHA. Understandably, this perspective places the VHA at the center of people and organizations with which the VHA is involved. These “stakeholders” represent the critical paths of information flow from the enterprise perspective. The following chart from the VHA Enterprise Architecture illustrates this perspective:[1]
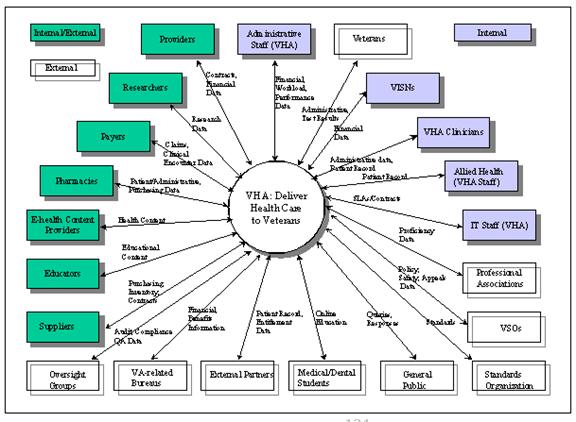 Figure 1 VHA
Figure 1 VHA
An alternative perspective – viewing from the edge – would be to put the individual at the center of the diagram. The spokes radiating out from the person would reflect the “stakeholders” in that person’s health, of which the VHA would be one spoke. There would be many other organizations, people, and enterprises which relate to that person’s health. VHA flips from being “inside” the circle of enterprises to being on the edge of its patient’s health activities.
HailStorm
Microsoft has announced a software architecture called HailStorm (to be released in late 2001) which reflects this perspective:[2]
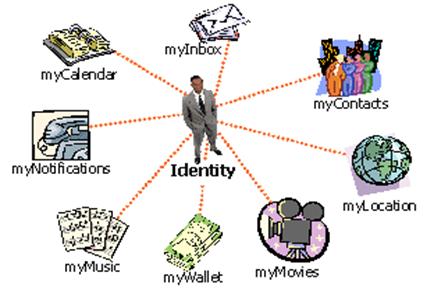
Figure 2 Microsoft HailStorm puts individual at center
Instead of people having to adapt to each technology, "HailStorm" services help different technologies cater to the user and provide a consistent experience across an individual's entire "personal network." "HailStorm"-based solutions allow users to manage and protect their personal information, as opposed to today's world in which it is scattered across the technology landscape, with no ability to control the privacy of their information. In addition, these solutions will allow different technologies to work together in tandem, saving the individual from acting as the integration point between all the technologies in their life.
Microsoft has designed an initial
set of generalized services which radiate around the individual: The initial
set of HailStorm services which have been announced
are:
·
myAddress - electronic
and geographic address for an identity
·
myProfile - name,
nickname, special dates, picture
·
myContacts -
electronic relationships/address book
·
myLocation -
electronic and geographical location and rendez-vous
·
myNotifications -
notification subscription, management and routing
·
myInbox - inbox items
like e-mail and voice mail, including existing mail systems
·
myCalendar - time and
task management
·
myDocuments - raw
document storage
·
myApplicationSettings
- application settings
·
myFavoriteWebSites -
favorite URLs and other Web identifiers
·
myWallet - receipts,
payment instruments, coupons and other transaction records
·
myDevices - device settings,
capabilities
Using Hailstorm, an appointment with the VHA could be sent to to the veteran’s “myCalendar.” This would then appear on the person’s time management system, whether is was a personal computer, PDA, cell phone, web site, or paper-based postal mail notification. The flexibility to choose how and where to direct these appointments would be controlled by the individual, not the enterprise.
From the enterprise architecture perspective, this could also make things more flexible. VHA would only have to issue an appointment notification in a standard format, it would not have to be concerned about how to present it on a veteran’s appointment system.
Some possible uses of HailStorm for VHA might be:
|
HailStorm Service |
Possible use by VHA |
|
myAddress |
Standard VA mailing, email, fax, and other contact
information |
|
myProfile |
Specific VA information, relating to edibility, Identity
presented to others (filtered by contacts), such as anonymous, pseudonymous,
or identified. |
|
myContacts |
VHA health team, contact information. Entry point for trust network. |
|
myNotifications |
Health events, annual exams, vaccinations, notices about
drugs, health reminders |
|
myInbox |
Integrated patient communications system, discussion
management, on-line support groups, knowledge base alerts |
|
myCalendar |
Appointment scheduling, medications, refills, lab tests |
|
myDocuments |
Folder could be set up for VA information; e.g., copies of
Health e-vet info could be stored there.
A standard folder definition could be used to store patient info for
allergies, H&P, etc. |
|
myApplicationSettings |
For VA application software, health e-vet settings |
|
myWallet |
To hold VA Dollars (see “complementary currency for
Veterans” in this paper) |
Figure 3 Possible Ways of Applying HailStorm to VHA
There are many VHA functionalities which could fit directly into the HailStorm model. It is also possible to think of the VHA as extending the the model. For example, Health e-Vet could be a part of a service (myHealth?) which would communicate information with the individual’s health service. This information would then automatically be integrated with all of the other provider’s health information.
Another idea would be to create a “myVA” service which serves the needs of veterans from the
department as a whole.
Comparison of Hailstorm with original DHCP design concepts
There are a
number of aspects of HailStorm which are parallel to
DHCP design concepts from the early 1980’s.
For example:
|
HailStorm Service |
HailStorm Description |
DHCP Kernel Service/concept |
|
myAddress |
electronic and geographic address for an identity |
Kernel User Parameters |
|
myProfile |
name, nickname, special dates, picture |
Kernel User Parameters |
|
myContacts |
electronic relationships/address book |
|
|
myLocation |
electronic and geographical location and rendezvous |
|
|
myNotifications |
notification subscription, management and routing |
MailMan Inbox-integrated
messaging, discussions, FileMan updates, alerts, Pendex |
|
myInbox |
inbox items like email and voice mail, including existing
mail systems |
MailMan Inbox |
|
myCalendar |
time and task management |
“Pendex” system- an integrated
system to track pending things for both the user, as well as patient-oriented
events for which the provider may be involved. |
|
myDocuments |
raw document storage |
FileMan |
|
myApplicationSettings |
application settings |
Kernel User parameters |
|
myFavoriteWebSites |
favorite URLs and other Web identifiers |
Universal NameSpace, in which
domain name would be pre-pended to FileMan
reference to communicate across all sites.
This created a Universal connectivity of all DHCP web sites |
|
myWallet |
receipts, payment instruments, coupons and other
transaction records |
|
|
myDevices |
device settings, capabilities |
Personalized user kernel parameters. |
Comments on SOAP, XML, and DHCP Kernel Architectures
SOAP (Simple Object Access Protocol) is a key protocol used by HailStorm for communicating between servers. It allows transactions to flow between web servers as well as via electronic mail messages.
There are many similarities between this approach and the architectural concepts built in to the early architecture of DHCP in the 1980’s. At that time, I was active in the design of the kernel, the FileMan, and MailMan. I have not kept current with the evolution of the system, but I suspect that there are still some features in the DHCP code which may be applicable. If not, the concepts may still have some potential.
The original MailMan was designed in 1984 as a network transport tool as well as many other things. It was designed in an era which required the use of 1200 baud autodial modems. Although this design is very old and based on obsolete technology, many of the concepts may be relevant to day. Here are some issues which may be relevant.
|
G.<name> |
Address a message to a group, as defined in the group file
of the destination’s GROUP file. |
|
O.<name> |
Address a message to an option on the destination’s menu
system. Thus, one site could send a message to another site’s computer. Note that if this capability still exists,
it could be connected to the SOAP process relatively easily, allowing
traditional DHCP systems to participate in SOAP exchanges through email. |
|
P.<name> |
Address a message to a patient. The original MailMan
concept was to extend mail service to every patient in the VA, and to use
this as a point of connection for patient-related communication and
tracking. Patients who did not have
access to email (this was in 1983) would get their mail digested and sent out
via paper mail. Patients were to get
separate baskets for appointments, correspondence, etc. |
|
<name> (no
prefix) |
Address mail to a MailMan
user. <name>
could include the “@” syntax, which would route the message to any other RFC
822 mail system address. |
|
F.<reference> |
This was part of a “universal namespace” concept which was never implemented. <reference> was to be a syntax consisting of the VA domain name followed by a FileMan reference for specific data. This provided a means of referencing any DHCP site from anywhere else. The web’s URL (universal resource locator) was a much more powerful definition of this idea. |
|
Pendex |
This was the name of a concept I was considering, but never put into code. The term stood for “Pending Index” and was to have been implemented as a form of cross referencing files by things which were pending. The pendex was to be organized by date and a code, indicating what to do if a scheduled event occurred and the event was not cleared. (Generating a MailMan message was one option). This would have allowed the system to track events which didn’t occur, such as missed appointments, refills not filled, lab tests not read, etc. The Pendex could be integrated into a notification system. In many cases, things which do NOT occur are more important than those which do occur. Transaction processing technology is largely based on tracking what does occur, leaving it difficult to track missing activities. Being able to post the expectation of an activity and then being notified of its non-occurrence would be a powerful architectural tool. This could have particularly strong implications for patient safety activities. |
|
FileGrams |
Filegrams were messages of FileMan data which were formatted according to the DIQ program format of <name>=<value>. XML provides a similar function. |
|
Data Dictionary |
There is almost a one-to-one mapping between the XML DTD (Document Type Descriptor) and the FileMan data dictionary. |
Industry Controversy over HailStorm Architecture
The HailStorm approach has brought considerable controversy as to the degree to which the architecture will be “open to customers but closed to competitors.” There are those who fear that the approach may be built in to the Microsoft operating systems so deeply that it would put competitors at a disadvantage:
Even before Microsoft
announced its new online services plan — dubbed Hailstorm — on Monday, some of
the company's leading competitors were quietly registering complaints about the
effort with government antitrust regulators.
The competitors, including AOL Time Warner and Sun Microsystems, allege that Hailstorm and other pieces of Microsoft's .Net initiative are designed to limit their access to customers and further leverage Microsoft's dominant Windows market share.
On Friday, AOL/TW officials
had a breakfast briefing with several state attorneys general involved in the
government's pending antitrust lawsuit against Microsoft, which is under review
by the U.S. Court of Appeals for the
In keeping with VHA’s role as a federal agency, it would be in a position to drive an open standards approach to the use of HailStorm for general use. If Microsoft chooses to make HailStorm a publicly accessible tool, then it could be of great use to VHA. If however, it becomes “open for users, but closed for competitors,” then its applicability for VHA would have to be assessed accordingly.
The obvious question is "Can a HailStorm transaction take place without talking to Microsoft owned or licensed servers?" The answer seems to be no, for two, and possibly three, reasons.
· First, you cannot use a non-Passport identity within HailStorm, and at least for now, that means that using HailStorm requires a Microsoft-hosted identity.
· Second, you cannot use a non-Microsoft copyrighted schema to broker transactions within HailStorm, nor can you alter or build on existing schema without Microsoft's permission.
· Third, developers might not be able to write HailStorm services or clients without using the Microsoft-extended version of Kerberos.[4]
Patient Flow vs. Provider Flow
If we look at health care as a flow of activities, we find a kind of relativity. From one perspective, the provider is fixed in space and the patients flow through the clinic, hospital, or organization. From the other perspective, the patient is fixed in space and the providers flow by. This may be illustrated as follows:
|
|
Enterprise-Centric |
Patient-Centric |
|
What is fixed |
The |
The Patient |
|
What moves |
Patients flow past the enterprise |
Providers flow past the patient |
|
Point of Reference |
Provider is fixed point of reference |
Patient is fixed point of reference |
|
Information Architecture |
|
Personal Information Space |
|
Clusters of information |
Departments, functional areas, diseases, protocols |
Areas of interest; communities of trust; family, career, geography, access |
|
Duration |
Encounter; “longitudinal” information for 1-50 years |
Lifelong; evolving with age, interest, health issues |
|
Information storage |
Organized along enterprise and industry and enterprise definitions |
Organized according to flow of interests, activities. |
To extend this line of thinking even further, the person at the center may have many things other than health care activities and interests to contend with. A doctor’s appointment is not an independent activity, for example. Other appointments must be checked, and the fact that an appointment has been made relates to other future appointments. Health care activities become only one aspect of a person’s electronic records, radiating from their personal information spaces.
Technology allows these individuals may connect in new ways. This can lead to the emergence of new health benefits as each can reinforce the health activities of others.
2. Health and the Network Effect
One of the more powerful concepts emerging from the Internet is the “network effect.” The value of a network to a given participant increases as the number of others on the network increases. For example, when fax machines were rare, each new fax machine increased the value of each existing fax machine. The more machines were available to communicate with, the more value the each became.
A critical perspective is, how do we use the dynamics of the network effect to improve veteran’s health? What kinds of things can be done to create self-propelling, self-organizing activities which amplify health?
In order to employ the network effect, we need connectivity and scalability. The technology for connectivity is advancing rapidly. Our understanding of scalability, however, is sometimes lagging our ability to connect. We still often think of systems from a hierarchical, enterprise perspective rather than the individual customer perspective.
In order to
evaluate activities for potential network effects, we need to take a fresh look
at health care. One way is to look at a
spectrum of activities at different scale.
A Spectrum of Health Activities
It is
interesting to look at a broad range of activities relating to the VHA’s mission to tend to the health of
|
Level |
Description (approximate benefit/cost) |
Sample Activity |
|
1 |
Nationwide benefit |
Replicates successful activity which grows to broad self-sustaining effectiveness assisting at national level (Viet Nam Veteran’s outreach clinics, Mothers Against Drunk Driving, Alcoholics Anonymous, etc) |
|
2 |
Community benefit |
Volunteerism, building community for increased health capital |
|
3 |
Small group benefit |
Start/lead self-help group |
|
4 |
Personal benefit |
Participate in self-help group, volunteer in community activities |
|
5 |
No Cost |
Hope, optimism, family, strong social network, positive outlook, healthy lifestyle, exercise, spiritual/religious strengths. |
|
6 |
$1 cost |
Vitamins, over the counter medications |
|
7 |
$10 cost |
Medical office visit, health club visit |
|
8 |
$100 cost |
Minor office procedure, vacation to reduce stress |
|
9 |
$1,000 cost |
MRI, office procedures |
|
10 |
$10,000 cost |
Hospitalization, simple surgery |
|
11 |
$100,000 cost |
Major surgery, bone marrow transplant |
|
12 |
$1,000,000 cost |
Cronic disease care, trauma, drunk driving accidents, spinal cord injury |
|
13 |
$billions+ |
Becoming first patient for a global epidemic, “patient zero” of HIV/AIDS |
Figure 4 Spectrum of Health Activities
This spectrum provides a framework for looking at opportunities for applying Information and Communications Technologies to the VA. The focus of Information technologies within the VHA is typically at levels 6-12 on the above spectrum. Levels 1 through 5 typically lie outside typical operations in the VHA.
How Cost/Benefit Analysis can Override Human Values
A recent
study by Arthur D. Little International sponsored by Phillip Morris concluded
that smoking was beneficial to the country, because premature deaths caused by
smoking saved the health care system $1227 each time a patient died prematurely.[5] Phillip Morris later apologized for
publishing the study. Sr. Vice President
Steven Parrish said that the funding of the study "exhibited
terrible judgment as well as a complete and unacceptable disregard of basic
human values.”[6]
This
study was particularly flagrant in its use of economic cost/benefit analysis to
override “basic human values.” However
blatant this study was, its methodology was not that different from most
economic analyses of health care activities.
If we
want to optimize the system for lowest cost, we can simply cut expenditures to
zero. “Everyone is going to die sooner
or later anyway,” is the cost-cutting extreme position. The extreme benefit position – trying to
defeat death – would end up with the nation’s GDP spent on life support for the
elderly, maximizing national longevity.
The discussion becomes one of “optimizing” some level of cost and
benefits between these two polarities.
It is as if there is a single line connecting the two options, and our
decision is “what percentage of the GDP should we spend minimizing costs versus
maximizing benefits.”
Human values are not collected at the transaction processing level. Our information systems monetize interaction according to predefined categories, then aggregate them into ever larger accounts as they work their way up to decision makers. Non-economic values, if they are considered at all, are applied separately to the process.
Limits of Economic Analysis of Health Care
The currency by which we do economic analysis is usually the dollar or its equivalent. Interactions are monetized by attaching a dollar amount to them, then added up to create a total cost. Kindig[7] makes extensive use of this form of analysis. However, there are a wealth of spoken or unspoken assumptions underlying this form of analysis. Some of the assumptions made in this study are:
1.
That
health can be purchased
2.
That
financial incentives drive health care
3.
Health
care is a matter of a “system” doing things to a “patient.”
4.
That
health care can be understood as the supply and demand of a scarce commodity.
5.
That we
are dealing with an “industry” in which producers “provide” health and people
“consume” it.
6.
That patients are only consumers of health, not also
producers.
7.
Decompositional
analysis is a way of understanding the health care system
8.
That the
process of analysis does not change the system being understood.
9.
That the
system is linear
10.
That
inputs don’t interact.
11.
That it
is possible to define health meaningfully across a whole population.
12.
That
this definition can be used to drive an aggregation of activities.
13.
That it
is possible to maximize health through coordination, planning, and management.
14.
That the
patient’s sense of self is not a factor in the efficacy of the intervention
15.
That
greater measurement with greater precision will converge on greater
understanding of the phenomenon being studied.
16.
Categorized
transactions can be “rolled up”
17.
That
there is a specific scale and “yardstick” with which we can measure health care
18.
That we
can manage the system by understanding and defining its problems.
19.
The placebo effect, mind-body interaction, racial, cultural and ethnic
backgrounds, personal belief system, and family factors relating to a person’s
health process are outside of “normal” medicine.
20.
That the system can look ahead and understand future consequences of
today’s activities.
21.
That the “law of increasing return” is not evident in health
Costs are more easily quantified and aggregated, while benefits do not necessarily have specific monetized effects.
How Currency Shapes Analysis
At the core of these economic analyses is the notion of money – the currency by which the decisions and tradeoffs are made. Rather than comparing apples and oranges, everything is converted to money. Computers are able to process transactions, add them up, and store them in data bases. A fundamental model of information technology is transaction processing of transactions monetized in a specific currency.
Bertrand Lietear, one of the designers of the Euro, speaks of the impact of the type of currency used for exchange:
”The type of currency used in a society encourages – or discourages – specific
emotions and behavioral patterns. Our
prevailing system [of world currencies] is an unconscious product of the modern
Industrial Age world view, and it remains the most powerful and persistent designer
and enforcer of the values and dominant emotions of that age…currencies were
designed to foster competition among their users, rather than cooperation…money
is a modern society’s central information system, akin to the nervous system in
our own bodies.”[8]
The type of currency used in health care decisions, such as the Czech koruna (equivalent to dollars) used in the Phillip Morris study, has a dramatic influence in our ability to communicate human values in our decisions. The numbers say one thing, and our decision makers must apply values from another perspective. This creates a built in conflict between our information processing systems and our value systems. The gap between “what the numbers say” and values is an ongoing problem. In particular, today’s currencies are designed from the perspective of scarcity – money is a scarce resource. However, health can be viewed according to the economics of plentitude – everyone can get healthier, and, in so doing, make everyone else a little healthier. What would a currency which dealt with Veteran’s Health look like?
3. Complementary Currencies for Health
Dee Hock, founding CEO of Visa International, spoke of how credit cards have changed the concept of money. “Money has evolved from shells to green paper to the artful arrangement of binary digits.”[9] Lietear presents a way to more closely relate our values and our currency – the use of “complementary currencies” to supplement or replace traditional money. For example, Frequent flier miles as a form of complementary currency, creating value and customer loyalty. There is also a wealth of other complementary currencies active today, some of which are used directly for health purposes:[10]
- Japanese Healthcare Currency. An application of a specialized
“healthcare currency” operating at the national level in
- Time Dollars Time Dollars are a
tax-exempt kind of money that empowers people to convert their personal
time into purchasing power by helping others and by rebuilding family,
neighborhood and community. An hour helping another earns One Time
Dollar. Time Dollars express four core values: 1) everyone has
strengths and assets; 2) raising children and building community is
valuable work;
3) mutual support is more powerful and empowering than one-way helping; and
4) trust is the basis for community.[11] - Elderplan Care Bank. Participants at this
The values of the community using
the currency are embedded in the currency itself. In
|
Currency |
Values |
|
Time Dollars |
Personal strengths, building community, mutual support, trust |
|
Care Bank |
Health |
|
Japanese |
Caring relationship |
Trust is integral to currencies. People who exchange goods and services for a dollar, for example, trust that they will be able to exchange the dollar with someone else. If this trust erodes, then the currency becomes worthless. There is nothing underlying the piece of paper which has value. A dollar bill says, “This note is legal tender for all debts, public and private” but that is all. If there were not a sufficiently large community of people who trusted that the dollar had value, the value of the dollar would plummet. On the other hand, this trust is subject to the law of increasing returns: the more people trust the currency, the more trustworthy it becomes for others to trust.
A complementary currency is based on the same principle: There must be a community of people who trust the currency. The more people trust it, the more attractive it becomes to others, which in turn creates additional trust.
Complementary currencies can be used in a variety of ways. For example,
- Complementary currencies make possible transactions and exchanges that otherwise would not occur…in one survey, more than half the people [using a complementary currency] started to provide services as a direct result of the availability of the complementary currencies in their community.
- This additional work and wealth is being generated where it is most needed without the need for taxes, government bureaucracy, and without creating the risk of inflation in the mainstream economy. Note that this is additional wealth, not the redistribution of existing wealth. Therefore complementary currencies are not a new form of welfare. Welfare is a compulsory transfer of resources from the rich to the poor via taxes. In contrast, the use of complementary currencies is voluntary for everyone; it creates new wealth, and – once started – becomes a completely self-funding mechanism to address many social problems without requiring permanent subsidies or taxes.
- Complementary currencies make not only social sense, but also business sense. They enable locally owned businesses to compete better against large chain distribution systems… in this sense, complementary currencies can also contribute to make the local economy more self-reliant, a modest but healthy counterweight to the relentless globalization of the economy.
The establishment of a complementary currency for the VA could create additional health and wealth in the Veterans community. It would do so in proportion to the increased trust and size of the community. This is a powerful way to exploit the network effect to improve Veterans health.
The Internet is a perfect technology for creating complementary currencies:
“It happens that some characteristics of the Net make it an ideal space where community-supporting currencies could happily thrive next to traditional national currencies, enabling a new symbiosis between the two approaches. Because Internet offers unlimited “space” and transcends natural and cultural boundaries, the electronic marketplace need not be limited to one exclusive currency system. New synergies between virtual communities and local communities would become possible, improving quality of life of the participating Netizens.”[13]
The health activities level 1-5 on figure 5 are all subject to the use of a VHA specific complementary currency. Because they are based on scalable benefits, rather than costs, their benefits would grow much faster than their costs. A complementary currency could be used to fuel this process.
VHA Health Bucks: A Scenario for a VA Complementary Currency
Imagine that the VA becomes the “central bank” for a new currency – “VA Health Bucks,” similar in concept to the Japanese health currency, Time Dollars, or the Care Bank. Initially, it is organized around volunteer efforts, with particular support from the Veteran’s Service Organizations. As its trustworthiness grows and the community using it grows, Veterans (and others) can earn them by volunteering their time in support of VA activities, and spend them on an increasing array of goods and services.
Over time, Veterans develop loyalty and trust in VA Health Bucks in much the same way that frequent fliers develop loyalty and trust in their mileage programs. As the currency and its community grow more trustworthy and more currency circulates, it plays an even stronger role. VA exchanges VA Health Bucks for discounts at the canteen, barber, or pharmacy. Veterans Service Organizations (VSOs) become part of the community, helping veterans as well as earning VA Health Bucks themselves.
Earning VA Health Bucks
Veterans might be able to earn VA Health Bucks in a variety of ways:
- Volunteering for service at a hospital
- Serving as a health buddy
- Organizing or supporting a physical or online support group
- Participating in research studies or questionnaires
- Adopting a healthier lifestyle, such as controlling weight, stopping smoking, abstaining from substance abuse.
- Donations and in-kind gifts
- Veterans Service Organizations support activities
- Donating Blood
- Complying with treatment programs
- As “bonuses” from clinicians as special patient motivators
Spending VA Health Bucks
Veterans would be able to use VA Health Bucks in a variety of ways:
- Discounts or free food at the Canteen
- Free services at the barber shop
- Discounted co-payments on prescriptions
- Free transportation services
- They could donate them to others
- Local merchants could redeem them, for example, free coffee at a coffee shop, recreation or dining discounts
- They could be saved for future needs, such as long term care or other unforeseen emergencies
- They
could be used for recognition awards and “premier” volunteer status
Health Buddies
One example of how the currency could work might be to support “Health Buddies,” in which one patient mentors another going through a similar operation. For example, John Smith has a hip replacement surgery. He volunteers to become a “health buddy” for Bill James who is undergoing the same operation. The two get to know each other; their interaction is mutually reinforcing:
1. Jim’s role as a mentor reinforces his post operative recovery process.
2. Bill sees a positive role model. “If Jim did it and is happy with the results, then so can I.”
3. Since Jim is seeing the operation for the second time, he knows what to expect, and may be able to make suggestions to the staff about how to improve the process for future patients.
4. Jim builds up VA dollars for use in the future, perhaps to assist in co-payments for prescriptions, or services or goods from the canteen.
5. The interaction builds community within the VA.
6. The interaction builds trust in the VA and in the Veteran population.
7. The interaction is scalable and low cost. There is little or no cost to the program; it can itself be run by volunteers earning VA Health Bucks.
8. The
interaction improves the health of both Jim and Bill.
The Health Bucks concept exploits the network effect. The more people use them, the more valuable they become. As they are tied to healthy behavior and activities, they are self-regulating. Over time, the system could become a completely self-funding mechanism to improve the health of veterans.
VHA Voluntary Program
The VA’s voluntary timekeeping software (see Appendix B) could be used as a foundation for the a complementary VHA health care currency. In a sense, it is already acting as a special purpose currency, exchanging volunteer hours for meal tickets and awards.
A more generalized approach would extend the concept to work off a common currency, such as the Health Bucks, which would be earned by specific activities, such as volunteering, making donations, etc. Instead of printing specific meal tickets for specific times, however, the Health Bucks would be given to the person to be used when and where they wished.
The concept of a health currency is a significant departure from the perspective currently encoded within the Voluntary system. The current system, for example, lists codes to define volunteer participation in the National Veterans Games. One section of this code (this is just a sample from 8 pages) is listed below:
|
604 604A 604P 604E 604M |
Hospitality Volunteer (Hotel) Morning
shift (6:oo am - Afternoon shift (12 Noon - 6:00 pm) Evening
shift ( Night shift (12 Midnight - 6:00 am) |
|
605 605A 605P 605E 605M |
Alternative Activities Volunteer Morning
shift (6:oo am - Afternoon shift (12 Noon - 6:00 pm) Evening
shift ( Night shift (12 Midnight - 6:00 am) |
|
606 606A 606P 606E 606M |
Souvenir Volunteer Morning
shift (6:oo am - Afternoon shift (12 Noon - 6:00 pm) Evening
shift ( Night shift (12 Midnight - 6:00 am) |
|
607 607A 607P 607E 607M |
Memorabilia Volunteer Morning
shift (6:oo am - Afternoon shift (12 Noon - 6:00 pm) Evening
shift ( Night shift (12 Midnight - 6:00 am) |
The
specificity of the coding system creates as many questions as it solves. What happens when someone works between two
shifts, for example from
An alternative currency would be able to track volunteer hours and convert them to a single VA Health Bucks currency, which could then be used for a variety of applications. Rather than having a separate set of programs designed to specifically print meal coupons for the canteen, the currency could be used by the volunteers as they needed. This would simplify the accounting, add flexibility, reduce staff accounting time, and create a larger community within which the currency was available.
Conclusion
Advances in
information and communications technologies over the next decade will introduce
dramatic changes beyond simple improvements in speeds and capacities. They will fundamentally change the way we
think about our systems and the relationship between the enterprise and the
customer. VHA should factor this into
its long range planning:
- VHA should study the possibility of using of Microsoft’s Hailstorm and/or its future competitors. The person-centric nature of the model, coupled with its service architecture, is attractive vehicle for many of the VHA’s information needs. However, HailStorm also introduces many issues relating to openness, competition, privacy, and security
- VHA
should consider creating a complementary currency for Veterans
health. This would position the VHA
as the “central banker” for a new currency, which would be used for
improving veterans’ health, encouraging volunteerism, greater involvement
of Veteran’s Service Organizations, growing the Veteran community,
improving trust, and engaging local merchants and organizations.
Acknowledgements
The author
wishes to recognize the contributions and discussions of
Appendix A: Microsoft HailStorm Architecture
Published: June 2001[14]
Key points:
|
|
HailStorm
 Microsoft is developing a
user-centric set of core XML Web services, codenamed "HailStorm",
which will be needed by many applications. HailStorm
services are oriented around people, instead of around a specific device,
application, service, or network. They put users in control of their own data
and information and allow you to access it at anytime from any device. They
also protect personal information by allowing the user to control who can have
access to their information and providing a new level of ease of use and
personalization. HailStorm services are just the
first set of the XML Web services being built by Microsoft.
Microsoft is developing a
user-centric set of core XML Web services, codenamed "HailStorm",
which will be needed by many applications. HailStorm
services are oriented around people, instead of around a specific device,
application, service, or network. They put users in control of their own data
and information and allow you to access it at anytime from any device. They
also protect personal information by allowing the user to control who can have
access to their information and providing a new level of ease of use and
personalization. HailStorm services are just the
first set of the XML Web services being built by Microsoft.
XML Web Services
XML Web services,
through the use of XML and SOAP, allow applications to talk regardless of
operating system or programming language via the Internet. With XML Web
services, not only can applications share data, but they can also invoke
capabilities from other applications without regard to how other applications
were build. Sharing data through XML allows them to be independent of each
other while simultaneously giving them the ability to loosely link themselves
into a collaborating group that performs a particular task.
Working with your consent
The HailStorm
services make user consent the basis for who can
access user information, what they can do with it, and how long they have
permission. In mid-March at the HailStorm Design
Preview, the first set of these XML Web services were showcased. Passport is
the first such service, giving developers the option to outsource their user
authentication services.
Passport to the future
Based on the Passport user
authentication system, HailStorm permits applications
and services to cooperate for the user's benefit, as well as allowing users,
groups, and organizations to share and collaborate. For instance, with HailStorm services, booking a flight using an online travel
reservation service becomes much simpler because with the user's consent, the
travel service automatically access the user's preferences and payment. If
you're traveling on business, and your company has travel policies you need to
adhere to, your individual affiliation with your company's HailStorm
group identity will make it possible for the travel service to automatically
show you only the choices that meet both your preferences and your company's
requirements.
Once you've chosen your
flight, the travel service can use HailStorm, with
your explicit permission, to figure out which calendaring service you use and
automatically schedule the itinerary onto your calendar, automatically updating
that itinerary and notifying you if your flight will be late. And through HailStorm, you can share that live flight itinerary with
whomever you're going to visit so that they will also know when and where to
expect you. The information in your HailStorm-enabled
calendar can then be accessed through your PC, someone else's PC, a smart
phone, a PDA, or any other smart connected device.
Initial Set of HailStorm
services
The initial set of HailStorm services will include:
myAddress - electronic and
geographic address for an identity
myProfile - name, nickname,
special dates, picture
myContacts - electronic
relationships/address book
myLocation - electronic and
geographical location and rendez-vous
myNotifications - notification
subscription, management and routing
myInbox - inbox items
like e-mail and voice mail, including existing mail systems
myCalendar - time and task
management
myDocuments - raw document
storage
myApplicationSettings - application
settings
myFavoriteWebSites - favorite URLs
and other Web identifiers
myWallet - receipts,
payment instruments, coupons and other transaction records
myDevices - device
settings, capabilities
Appendix B: VHA Voluntary Timekeeping Software System
Overview The Voluntary Timekeeping module automates the process of recording volunteer time at a medical facility. Volunteer hours can be recorded by the volunteers themselves which lightens workload on staff. This software allows volunteers to log themselves into the system in a language selected by the volunteer and then keeps track of their hours worked. The program can produce statistical reports detailing volunteer activities for a given time period or provide lists of any data stored in a master file, such as a meal list for Canteen Service. This software transmits time information to the Austin Automation Center (AAC).
Features
· Provides multi-lingual interaction with volunteers during log-in.
· Supports multiple division facilities.
· Electronically updates the AAC’s master file.
· Eliminates use of Generic Code Sheets module and/or FALCON for changes to AAC’s master file data.
· Displays or prints entire master record for a single volunteer.
· Provides local printing of address labels and telephone lists.
· Provides expanded field sizes for names and addresses.
· Reduces workload required to input mass award code changes.
· When using Auto Log-in, provides the ability to view list of volunteers currently on station.
· Enhances security for multiple division facilities.
· Automatically updates hours, years, and award information on a monthly basis from the AAC into a master file.
· Prints an individual meal ticket for the volunteer (using a small receipt printer) after Auto Log-in.
Appendix C: A Peer to Peer Health Care System
A
HEALTHIER CHIN[15]
Imagine going to an M.D. or clinic for the first time, and
during the examination, the doctor pulls up your entire health care
history—even though she had nothing to do with your previous treatment—all on a
PC. She can see that you visited a clinic
across town two years ago for a severe flu (and that the clinic ran some tests
to rule out infections); you went to an emergency room for a badly twisted
ankle; and you picked up a few extra pounds in the past year, which seems to be
making your blood pressure tilt higher.
Unless you carry around such
detailed records, you might forget an illness or a pattern of visits critical
to a diagnosis. The thought of putting such complete patient information at
doctors’ fingertips is why several
CHINs are
far from ubiquitous, but the ones that exist are usually built on a central data
warehouse. All health care providers in one county or geographic region that
contribute patient information can electronically access the entire range of
data. It’s a good idea, but in
Enter P2P. With it, the group could
avoid building and maintaining a pricey, complicated centralized database. With
$10 million in funding
Four institutions are already online, and the
rest are expected to follow by year’s end. “Let’s face it, in the
For example, a central index server
aggregates and tracks the various ways in which a patient’s name is listed by
participating institutions. For example, if a doctor types in J.G. Smith, the
server will search all of its computers and pull up John G. Smith and John
Smith. The doctor then can choose the correct records. Considering the critical
nature of the data,
Peer groups are nothing new for
doctors, although the contact is usually face-to-face. Yet it perhaps explains
why the new peer-to-peer arrangement for exchanging vital patient information
seems to be just what the doctor ordered.—SLRW